Glioma is the most common primary brain tumor in adults. While brain cancers are difficult to treat, detecting and removing the tumor as early as possible is crucial to optimizing prognosis.
Gliomas develop in the glial cells that surround neurons and help them function. Gliomas can affect motor and neurological abilities and functions, including cognitive functions. They may also affect the personality of the patient.
This type of tumor differs from so-called secondary brain tumors, which are metastases that develop from another cancer located in another organ. Glioma can affect people of all ages, including children, adolescents, and young adults.

Tumors with multiple forms and evolutions
Gliomas come in a variety of forms depending on the type of cell affected. Gliomas are divided into low-grade and more aggressive high-grade tumors.
The discovery of mutations in isocitrate dehydrogenase (IDH) in 2008 started a new era in the molecular classification of gliomas. Gliomas with IDH mutations (mIDH gliomas) are now known to be molecularly different than glioblastoma – the most aggressive form of glioma. There are two types of IDH mutant tumors: IDH mutant astrocytoma, and oligodendroglioma.
Most patients with IDH-mutant gliomas present to medical attention after a seizure3,4, or the tumors are discovered incidentally when brain magnetic resonance imaging (MRI) is obtained for evaluation of complaints unrelated to the tumor 5,6.
Key figures – in the US
The main forms of glioma
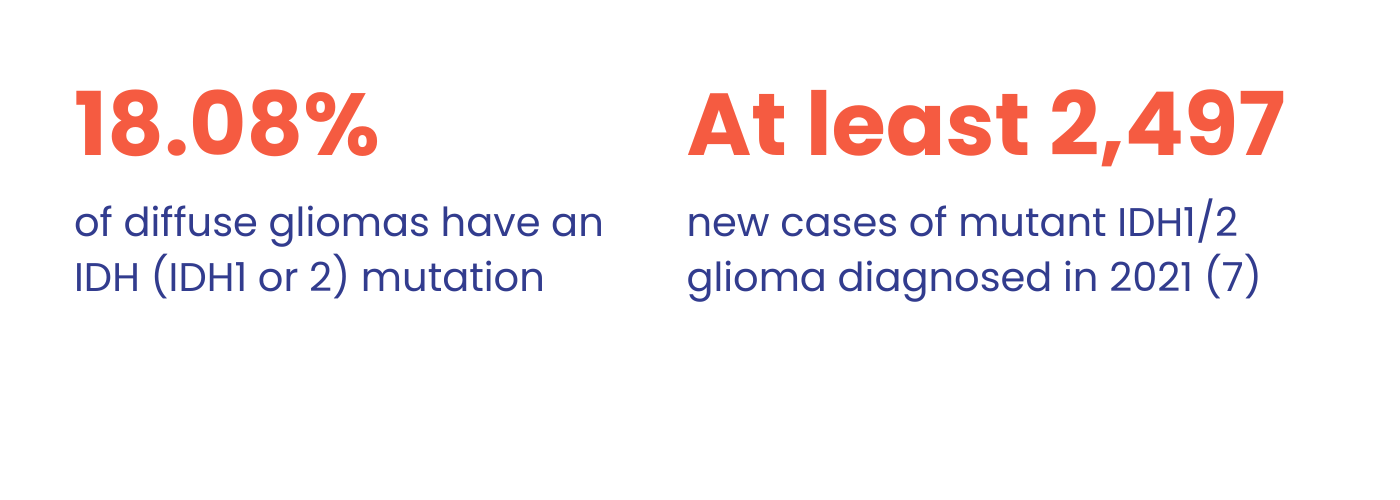
Establishing the IDH mutation status of these tumors is essential to both diagnosis and prognosis, per the 2021 WHO classification of Central Nervous System tumors and the National Comprehensive Cancer Network treatment guidelines, respectively. According to the 2021 WHO SNC tumors classification, adult-type diffuse gliomas are sub-divided into three categories:
- Oligodendroglioma, IDH-mutant and 1p19q-codeleted (grades 2-3)
- Glioblastoma, IDH-wildtype
- Astrocytoma, IDH-mutant (grades 2-4)
Illustrated infographic presenting the Glioma 2021 WHO grading
IDH mutation is now considered as the primary key driver of diagnosis and grading does not only rely on histology.
The challenge is therefore to detect the tumor, remove it and characterize it as early as possible. Hence the importance of identifying risk factors and recognizing symptoms.
Main risk factors and symptoms of glioma
To date, no precise cause of glioma has been identified. However, certain factors may increase the risk of developing a glioma:
- Age. Patients are young with a median age at diagnosis from 36 to 45 years (astrocytomas/ oligodendroglioma)1,8
- Exposure to ionizing radiation, particularly radiotherapy as part of cancer treatment.
- Certain hereditary syndromes or diseases.
Symptoms depend on tumor location, size and progression. There are a number of common signs that may indicate the presence of a glioma:
- Epileptic seizures: these are among the most frequent symptoms of gliomas, particularly low-grade ones.
- Neurological problems: vision problems, difficulty speaking or understanding, loss of strength or sensitivity in one part of the body, behavioral changes or irritability, memory loss, numbness or weakness in the lower part of the body.
- Symptoms associated with increased pressure in the brain: headaches, nausea, vomiting, double vision, drowsiness.
- Thromboembolic events (clot formation in the bloodstream): motor deficits and/or immobility.
These clinical signs should prompt the patient to seek prompt medical attention. They may also be the manifestation of other health problems. Only specific medical examinations can establish a precise diagnosis.
Glioma: about care
The molecular characterization, histology and grading of a glioma help doctors determine the appropriate treatment plan. IDH1/2m diffuse gliomas are not curable and mostly transforming into aggressive enhancing glioma10.
Initial management of IDH1/2-mutant adult-type diffuse glioma is surgical resection, when possible, which has retrospectively shown improvements in survival. Current post-operative standard of care for patients who are at risk of early disease progression is chemoradiotherapy11,12.
Treatment is associated with radiation-induced neurocognitive dysfunction, chemotherapy-associated DNA hypermutation and other toxicities11.
Patients with IDH1/2-mutant adult-type diffuse glioma may choose active observation (watch and wait) instead of chemotherapy or radiation therapy, if conditions permit11.
References:
[1] Ostrom QT et al. Neuro Oncol 2022;24( Suppl 5):v1 95
[2] Gatta G, van der Zwan JM, Casali PG, Siesling S, Dei Tos AP, Kunkler I, Otter R, Licitra L, Mallone S, Tavilla A, Trama A, Capocaccia R; RARECARE working group. Rare cancers are not so rare: the rare cancer burden in Europe. Eur J Cancer. 2011 Nov;47(17):2493-511. doi: 10.1016/j.ejca.2011.08.008. Epub 2011 Oct 25. PMID: 22033323.
[3] Schiff D. Low-grade gliomas. Continuum. 2015; 21(2 Neuro-oncology):345–354.
[4] Gonzalez Castro LN, Milligan TA. Seizures in patients with cancer. Cancer. 2020; 126(7):1379–1389
[5] Morris Z, Whiteley WN, Longstreth WT, Jr, et al. Incidental findings on brain magnetic resonance imaging: systematic review and metaanalysis. BMJ. 2009; 339:b3016.
[6] Opoku-Darko M, Eagles ME, Cadieux M, Isaacs AM, Kelly JJP. Natural history and growth patterns of incidentally discovered diffusely infiltrating lowgrade gliomas: a volumetric study. World Neurosurg. 2019; 132:e133–e139
[7] Ostrom QT, et al. J Neuro-oncol. 2023 Oct;25(Supplement_4):iv1-iv99.
[8] Miller JJ et al, Neuro Oncol , 2023 Jan; 25 (1):4 25
[9] Miller JJ et al. Neuro Oncol2023;noac207
[10] Youssef et al, Curr Neurol Neurosci Rep, 2020; 20(7): 21.
[11] Weller M et al. Nat Rev Clin Oncol 2021;18:170–86.
[12] NasanyRA et al. CurrNeurol NeurosciRep 2023;23:225–33.
NRD24-INST-ADV-034 09/2025